Abstract
Background: For newly diagnosed people with epilepsy (PWE), proper treatment is important to improve outcomes, yet limited data exist on markers of quality care.
Objective: Examine markers of quality care for newly diagnosed PWE.
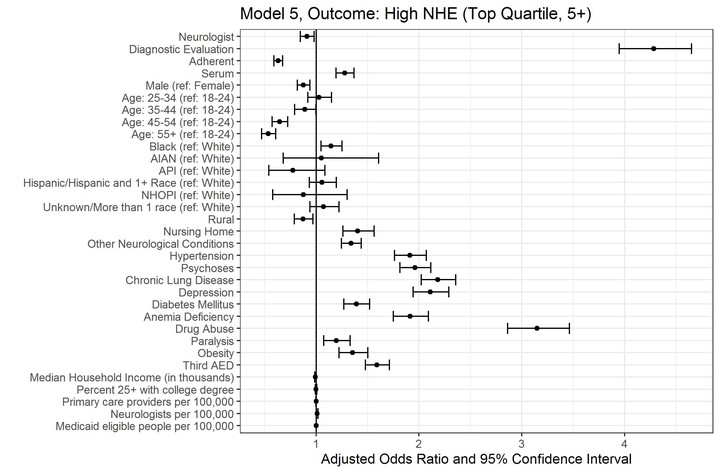
Methods: Using Medicaid claims data (2010-2014) for 15 states we identified adults 18-64 years of age diagnosed with incident epilepsy in 2012 or 2013. We built 5 sequential logistic regression models to evaluate: (1) seeing a neurologist; (2) diagnostic evaluation; (3) antiepileptic medication adherence; (4) serum drug levels checked; and (5) being in the top quartile of number of negative health events (NHEs). We adjusted for demographics, comorbidities, county-level factors, and the outcomes from all prior models.
Results: Of 25,663 PWE, 37.3% saw a neurologist, with decreased odds for those of older age, those residing in counties with low-density of neurologists, and certain race/ethnicities; about 57% of PWE received at least 1 diagnostic test; and nearly 62% of PWE were adherent to their medication. The most common comorbidities were hypertension (37.1%) and psychoses (26.9%). PWE with comorbidities had higher odds of seeing a neurologist and to have NHEs. Substance use disorders were negatively associated with medication adherence and positively associated with high NHEs.
Conclusions: There are notable differences in demographics among people with incident epilepsy who do or do not see a neurologist. Differences in NHEs persist, even after controlling for neurologist care and diagnostic evaluation. Continued attention to these disparities and comorbidities is needed in the evaluation of newly diagnosed PWE.
Wyatt P. Bensken, PhD
Research Investigator & Adjunct Assistant Professor of Population and Quantitative Health Sciences
My expertise is in the use of complex health care data, paired with traditional statistical and novel machine learning approaches, to identify opportunities to improve health, health care, and health outcomes for all.